Can Anxiety Cause High Blood Pressure?
Anxiety and stress can contribute to higher blood pressure readings.
When feeling anxiety, it is common to have a short-term increase in blood pressure. In response to a perceived threat, stress and fear can cause parts of the nervous system to become activated, raising heart rate and blood pressure. This is known as the sympathetic nervous system, or the “fight or flight,” system, which is controlled by adrenaline. Adrenaline will prepare you for battle, but it will also raise your blood pressure, heart rate, and make it harder to sleep. If you imagine a spectrum between being asleep and being awake, anxiety is being very awake, alert and reactive.
Our brains allow us to imagine anything – and this is a blessing and a curse, as we can also imagine what is not real or present. In anxiety disorders, these stress responses continue even when any threat has diminished. This can affect a person’s mental health, physical health, and quality of life. With such powerful imaginations, just thinking of a stressful meeting can cause the same response we would have to a physical threat – like a tiger in the jungle. A bit of anxiety is good to prepare, too much and performance diminishes. See article “Chess Is Best Played Calm.”
Perhaps not surprisingly, then, some research has found an association between anxiety disorders and hypertension, a condition of persistently high blood pressure.
Understanding the relationship between these conditions is important because of their significant prevalence among people in the United States. Around 19% of adults are believed to have or recently have had an anxiety disorder, and as many as 45% have hypertension. When left untreated, hypertension can heighten the risk of cardiovascular problems and kidney disease.
This post gives an overview of anxiety disorders and hypertension and goes into detail about how these two conditions may be linked. It also provides information about how they may be managed with both lifestyle changes and medications.
Overview of Anxiety Disorders
People with anxiety disorders experience profound feelings of worry or fear that regularly interfere with their everyday life and activities.
Virtually everyone has thoughts or feelings of anxiety from time to time. These worries may be driven by acute stress from things like work, health, or relationships.
But in people with anxiety disorders, fear and worry become chronic and don’t subside even when the source of stress is diminished. People with anxiety disorders typically focus undue attention on their worries, and these negative thoughts become more and more difficult to control over time. A bit of planning and preparation is always helpful, but a constant preoccupation with things going wrong, or bad outcomes, can be exhausting mentally, and also the cause of physical symptoms. In my work, people with anxiety are similar to a car without shock absorbers. Every bump is a big deal, and there are many bumps each day. This can lead to fatigue, burnout, and overall dissatisfaction with life. With a focus on the negative, people with anxiety see more of what is wrong rather than what is right, and life can begin to feel like a threat rather than a gift.
Types of Anxiety Disorders
Not all anxiety disorders are the same. Some of the main types of anxiety disorders and their key characteristics are:
- Generalized Anxiety Disorder (GAD): Persistent and excessive worry about various aspects of life, often without a specific cause.
- Panic Disorder: Recurring panic attacks that involve sudden feelings of intense fear.
- Social Anxiety Disorder: Strong fear of social situations due to concerns about being judged or embarrassed.
- Phobia-Related Disorders: Powerful, irrational fear of specific objects or situations (like flying, heights, or insects), leading to avoidance behavior.
- Separation Anxiety Disorder: Excessive fear of being away from certain people, most often seen in children but also in some adults.
Causes of Anxiety Disorders
The exact cause of anxiety disorders is unknown, but researchers have identified a number of risk factors that are associated with a greater likelihood of having an anxiety disorder.
For example, studies have observed a link between being exposed to higher levels of trauma and stress as a child and the development of generalized anxiety disorder (GAD). GAD is also more common in people whose tendency at a young age was to be shy when confronted with an unfamiliar situation. Some studies also suggest that genetics or a family history may be a risk factor for some anxiety disorders.
Symptoms of Anxiety Disorders
Anxiety symptoms can take many forms depending on the type of anxiety disorder and its severity.
Many of the most common symptoms affect thoughts and emotions. For example, people with anxiety disorders may have:
- A feeling of being on edge
- Restlessness
- Difficulty controlling negative thoughts or worries
- Irritability
- Trouble concentrating
- Trouble falling or staying asleep (waking after 4-5 hours)
In addition, they may have physiological symptoms felt directly in the body, including:
- Headaches
- Sweating
- Rapid pulse
- Upset stomach
- Muscle tension or pain
- Fatigue
- Trembling
- Chest pain or a feeling of weight on the chest
- Dizziness or lightheadedness
Frequently elevated stress hormones, like adrenaline and cortisol can lead to metabolic syndrome. This includes an increased risk of weight gain, high blood pressure, diabetes (or high blood sugar), and elevated cholesterol. Diminished sex drive is also seen, as people cannot relax in the moment. Substance use is more common as people look for ways to relax.
Tired but Wired
Sleeping problems are common among people with anxiety. This may involve difficulty falling asleep, staying asleep, or both. The inability to get good sleep can exacerbate other anxiety symptoms. People with anxiety commonly experience “battlefield sleep.” This is a vigilant sleep where it takes a while to fall asleep. You wake easily, with trouble falling back to sleep. People with this type of sleep usually get the bare minimum of 4-6 hours per night. While they can survive on this amount of sleep, it is not ideal for mental or physical health in the long term. We frequently treat patients with this type of condition, and it is essential to improve both daytime and nighttime symptoms to get things back on track. Better days make for better nights. And better nights make for better days. This sets up a virtuous cycle for people to improve remarkably.
Unfortunately, many people with anxiety disorders also experience depression. A focus on the negative, constant adrenaline spikes, catastrophic thoughts, and mounting fatigue can be exhausting and make days hard. Over time, these can lead to intense feelings of sadness which can then worsen anxiety’s impacts on sleep, mood, and concentration.

Overview of High Blood Pressure
As blood moves through blood vessels and arteries, it exerts pressure on the vessel and artery walls. This is known as blood pressure, which is measured in millimeters of mercury (mmHg) at two different times:
- Systolic blood pressure, which is measured when the heart beats
- Diastolic blood pressure, which is measured between heartbeats
A person’s blood pressure is expressed with these two numbers, listing the systolic pressure “over” the diastolic pressure. This is what it means when you hear two numbers like “120 over 80” to describe blood pressure.
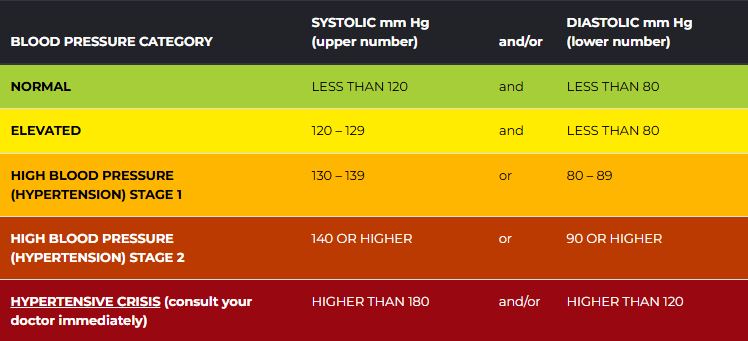
When blood pressure gets too high, it is known as hypertension. According to definitions from expert groups like the American Heart Association (AHA), hypertension occurs when the systolic pressure is 130 mmHg or higher or when the diastolic pressure is 80 mmHg or higher. A blood pressure chart from the AHA shows how the two blood pressure measurements influence your blood pressure category.
Blood pressure goes up and down at different times, so having high blood pressure at one moment does not necessarily mean that your blood pressure is always elevated. You may need multiple measurements at different appointments or even at home to be diagnosed with hypertension.
Controlling blood pressure is important because hypertension puts stress on the arteries and heart. Over time, this can damage vital organs, including the heart and kidneys. As a result, high blood pressure is a risk factor for heart disease, stroke, heart attack, and other cardiovascular problems.
The Relationship Between Anxiety and Blood Pressure
Although still not fully understood, experts believe that there is a connection between anxiety and blood pressure. Adrenaline, nor-adrenaline (norepinephrine or NE), and cortisol play a huge role.
In the short term, anxiety may provoke immediate rises in blood pressure. This is because stressors and the external environment can influence blood pressure.
For example, some people experience white coat hypertension, which is when blood pressure readings are normal at home but elevated during medical appointments.
Another condition marked by episodic increases in blood pressure is called labile hypertension. Some experts report that labile hypertension is more common among patients who are nervous or anxious.
Over a longer time horizon, there may be a link between ongoing problems with anxiety and hypertension. More research is needed, but some studies suggest that people who have persistent anxiety are at a higher risk of having chronic high blood pressure.
Mechanisms Behind Stress-Induced Blood Pressure Increases
It is normal for blood pressure and heart rate to rise when encountering a scary or stressful situation. This occurs as part of the “fight-or-flight” response, which is driven by the sympathetic nervous system.
This part of the nervous system operates automatically and sends signals throughout the body, including to the heart and blood vessels. Activation of the sympathetic nervous system can also trigger the release of certain hormones, such as cortisol, that are associated with the body’s stress response.
As a result, feelings of anxiety and worry may provoke immediate increases in blood pressure. In some cases, including in people with labile hypertension, this happens frequently and can involve substantially elevated blood pressure levels.
Some evidence indicates that certain people have higher blood pressure reactivity when facing mental stress. This means that they are more susceptible to their blood pressure rising when they are worried or anxious. This may be related to changes in neural activity in brain regions involved in processing stress and managing the sympathetic nervous system, such as the brainstem, amygdala, and hippocampus.
Fundamentally, if someone’s blood pressure tends to spike too easily (driving or in the doctor’s office) this may be a hint at a type of “reactivity” that we see in anxiety disorders. Anxious people tend to be jumpy, and so is their blood pressure and heart rate.
Symptoms of High Blood Pressure Due to Anxiety
Elevated blood pressure is often asymptomatic. In fact, because of the lack of symptoms, people frequently don’t know that they have hypertension, leading it to sometimes be called a “silent killer.”
This means that high blood pressure from stress or anxiety may not have any apparent symptoms. However, other signs of a stress response may correspond with an increase in blood pressure. These could include reactions like:
- Heart palpitations or a rapid pulse
- Headache
- Warmth and redness usually affect the face
- Chest pressure, heaviness
- Frequent urination
Anxiety-driven increases in blood pressure may also be accompanied by symptoms of anxiety, including feeling edgy or irritable.
Managing Anxiety to Control Blood Pressure
There are several types of treatment that can help treat anxiety disorders. More research is needed to know how exactly these treatments for anxiety disorders affect blood pressure levels.
Potential treatments for anxiety can include:
- Therapy: Various types of psychotherapy, including talk therapy like cognitive behavioral therapy (CBT), can help people reorient negative thinking that contributes to anxiety disorders.
- Stress management: Learning to prevent, reduce, and better respond to stress can help minimize the symptoms of anxiety. Examples of stress management approaches include breathing and relaxation techniques, physical exercise, and mindfulness meditation.
- Medications: Prescription drugs can help some people reduce the symptoms of an anxiety disorder. Types of medications that may be prescribed are benzodiazepines, other anti-anxiety drugs, and certain antidepressants. SSRIs or selective serotonin reuptake inhibitors are a commonly used medication for anxiety, and are quite effective. Fundamentally, these medications make it easier to “let things go,” which can be very helpful when someone thinks and reacts too much.
It is important to talk with a doctor about the most appropriate treatment for anxiety in light of your symptoms and overall health, including other health conditions like hypertension.
Treatments and Remedies for High Blood Pressure
There are a number of different ways to help manage blood pressure. It is best to work with a doctor to develop a plan that is tailored to you and that you can stick with over time.
Taking steps to treat hypertension is important because of the potential long-term health complications that can develop as a result of high blood pressure.
Lifestyle Changes for Better Blood Pressure Control
Making lifestyle changes can go a long way to enhancing blood pressure control. Some of the most beneficial things that you can do for heart health and blood pressure management include:
- Blood pressure monitoring: Taking regular blood pressure readings at home can help you monitor changes over time.
- Eating a balanced diet: Eating a healthy diet, including vegetables and fruits, can contribute to a healthy weight and better blood pressure control. The Dietary Approaches to Stop Hypertension (DASH) diet includes some specific recommendations for managing blood pressure.
- Cutting down on salt: Excess sodium can push up blood pressure numbers, so managing salt intake may be helpful. This is a component of eating plans like the DASH diet.
- Minimizing alcohol consumption: To help regulate blood pressure, it is best to avoid having more than two alcoholic drinks per day.
- Quitting smoking: Smoking harms the cardiovascular system, so quitting smoking can be a major step in lowering blood pressure and improving heart health.
- Sleep: Making sleep a priority, with regular bed and wake times, and a 1-2 hour, “cool down,” period before bed (without screens, reading, relaxing). Allowing an 8-hour opportunity for sleep is important. Better sleep makes for less anxiety.
- Engaging in regular physical activity: Staying physically active can help control blood pressure and offer a range of other important health benefits.
- Managing stress: Strategies for relaxation and stress reduction can help blunt the impact of stress on blood pressure. Being mindful and avoiding triggering situations can help, but checking in with your own responses to stress is important too. Having awareness that you may overthink, or overreact is important, and sometimes we need to catch ourselves in these most difficult moments. Practice letting go of the smaller stuff, so you get better when things get hard. Meditation always helps, even 5 to 10 minutes a day. Think of it as an exercise for calming the mind, and bringing thoughts back to breath.
In some cases, lifestyle changes alone are enough to manage hypertension. Some of these same habits, such as exercise and stress reduction, are also helpful for addressing anxiety.
Medications for High Blood Pressure
Depending on your blood pressure levels, your doctor may recommend that you take blood pressure medication.
There are multiple types of medications that can be prescribed for hypertension.
- Diuretics, which are also known as water pills and are designed to reduce the amount of fluid in the blood vessels.
- ACE inhibitors, which stop the production of a hormone that causes the narrowing of the blood vessels
- Angiotensin II receptor blockers, which restrict the effect of that same hormone
- Calcium channel blockers, which help slacken blood vessels
- Alpha blockers, which help widen blood vessels
- Direct vasodilators, which are another drug to make blood vessels wider
- Beta blockers, which reduce the activity of the sympathetic nervous system
With a range of medicines available, doctors may try several different options and dosages to see which offers the best blood pressure control with the fewest side effects. For some people, it may be necessary to take more than one drug to effectively treat hypertension.
When to Seek Medical Advice
You should contact your doctor if you have any symptoms of an anxiety disorder. While it’s normal to sometimes have worries and concerns, you should get medical advice if persistent fears or worries are affecting your mental health, mood, or day-to-day life.
You should also talk to your primary care provider or other healthcare provider if you have had high blood pressure readings or have questions about your cardiovascular health.
During an appointment, your doctor can ask questions about your symptoms, review your overall health and history of other health conditions, and provide actionable information to guide your lifestyle choices and any appropriate treatments for you.
While many of the suggested lifestyle changes for anxiety and hypertension can be made on your own, it is always best to consult with a doctor for guidance when considering any major change to your diet, physical activity, or other important health habits.
Sources and Works Consulted
A.D.A.M. Medical Encyclopedia. (2022, October 25). DASH diet to lower high blood pressure. MedlinePlus: National Library of Medicine. Retrieved on December 11, 2024, from https://medlineplus.gov/ency/patientinstructions/000770.htm.
A.D.A.M. Medical Encyclopedia. (2023, May 10). Generalized anxiety disorder. MedlinePlus: National Library of Medicine. Retrieved on December 11, 2024, from https://medlineplus.gov/ency/article/000917.htm
American Heart Association. (2024, May 7). Managing stress to control high blood pressure. Retrieved on December 11, 2024, from https://www.heart.org/en/health-topics/high-blood-pressure/changes-you-can-make-to-manage-high-blood-pressure/managing-stress-to-control-high-blood-pressure
American Heart Association. (2024, May 17). Understanding blood pressure readings. Retrieved on December 11, 2024, from https://www.heart.org/en/health-topics/high-blood-pressure/understanding-blood-pressure-readings
American Heart Association. (2024, May 23). What is high blood pressure? Retrieved on December 11, 2024, from https://www.heart.org/en/health-topics/high-blood-pressure/the-facts-about-high-blood-pressure
Baldwin, D. (2024, August 26). Generalized anxiety disorder in adults: Epidemiology, pathogenesis, clinical manifestations, course, assessment, and diagnosis. In: M. B. Stein (Ed.). UpToDate. Retrieved on December 11, 2024, from https://www.uptodate.com/contents/generalized-anxiety-disorder-in-adults-epidemiology-pathogenesis-clinical-manifestations-course-assessment-and-diagnosis
Basile, J. N. & Bloch, M. J. (2024, October 18). Overview of hypertension in adults. In: W. B. White (Ed.). UpToDate. Retrieved on December 11, 2024, from https://www.uptodate.com/contents/overview-of-hypertension-in-adults
Bloch, M. J. & Basile, J. N. (2024, February 12). Patient education: High blood pressure, diet, and weight (Beyond the Basics). In: W. B. White (Ed.). UpToDate. Retrieved on December 11, 2024, from https://www.uptodate.com/contents/high-blood-pressure-diet-and-weight-beyond-the-basics
Chen, X., Xu, L., & Li, Z. (2022). Autonomic neural circuit and intervention for comorbidity anxiety and cardiovascular disease. Frontiers in Physiology, 13, 852891. https://doi.org/10.3389/fphys.2022.852891
Chu, B., Marwaha, K., Sanvictores, T, Awosika, A. O., & Ayers, D. (2024, May 7). Physiology, stress reaction. StatPearls. Retrieved on December 11, 2024, from https://www.ncbi.nlm.nih.gov/books/NBK541120/
Coon, E. (2023, July). Overview of the autonomic nervous system. Merck Manual Consumer Version. Retrieved on December 11, 2024, from https://www.merckmanuals.com/home/brain-spinal-cord-and-nerve-disorders/autonomic-nervous-system-disorders/overview-of-the-autonomic-nervous-system
Egan, B. M. (2024, October 8). The prevalence and control of hypertension in adults. In: W. B. White (Ed.). UpToDate. Retrieved on December 11, 2024, from https://www.uptodate.com/contents/the-prevalence-and-control-of-hypertension-in-adults
Levenson, J. L. (2024, July 18). Psychological factors affecting other medical conditions: Clinical features, assessment, and diagnosis. In: J. Dimsdale (Ed.). UpToDate. Retrieved on December 11, 2024, from https://www.uptodate.com/contents/psychological-factors-affecting-other-medical-conditions-clinical-features-assessment-and-diagnosis
Lim, L. F., Solmi, M., & Cortese, S. (2021). Association between anxiety and hypertension in adults: A systematic review and meta-analysis. Neuroscience and Biobehavioral Reviews, 131, 96–119. https://doi.org/10.1016/j.neubiorev.2021.08.031
Mann, J. FE. (2023, November 3). Patient education: High blood pressure in adults (Beyond the Basics). In: W. B. White (Ed.). UpToDate. Retrieved on December 11, 2024, from https://www.uptodate.com/contents/high-blood-pressure-in-adults-beyond-the-basics
Mann, J. FE. (2023, November 3). Patient education: High blood pressure treatment in adults (Beyond the Basics). In: W. B. White (Ed.). UpToDate. Retrieved on December 11, 2024, from https://www.uptodate.com/contents/high-blood-pressure-treatment-in-adults-beyond-the-basics
Mann, S. J. (2023, January 10). Labile hypertension. In: W. J. Elliott (Ed.). UpToDate. Retrieved on December 11, 2024, from https://www.uptodate.com/contents/labile-hypertension
Nagai, M., Kato, M., & Keigo, D. (2022). Anxiety and hypertension in the COVID-19 era: How is the central autonomic network linked? Hypertension Research, 45(5), 922–923. https://doi.org/10.1038/s41440-022-00864-w
National Institute of Mental Health. (2024, April). Anxiety Disorders. Retrieved on December 11, 2024, from https://www.nimh.nih.gov/health/topics/anxiety-disorders
National Institute of Mental Health. (n.d.). Statistics: Any Anxiety Disorder. Retrieved on December 11, 2024, from https://www.nimh.nih.gov/health/statistics/any-anxiety-disorder
Suni, E. (2024, April 23). Anxiety and sleep. A. Dimitriu (Ed.). Retrieved on December 11, 2024, from https://www.sleepfoundation.org/mental-health/anxiety-and-sleep
United Kingdom National Health Service. (2024, October 22). Generalised anxiety disorder (GAD). Retrieved on December 11, 2024, from https://www.nhs.uk/mental-health/conditions/generalised-anxiety-disorder-gad/
UpToDate. (n.d.). Patient education: Controlling your blood pressure through lifestyle (The Basics). Version 15.0. Retrieved on December 11, 2024, from https://www.uptodate.com/contents/controlling-your-blood-pressure-through-lifestyle-the-basics
UpToDate. (n.d.). Patient education: Generalized anxiety disorder through lifestyle (The Basics). Version 15.0. Retrieved on December 11, 2024, from https://www.uptodate.com/contents/generalized-anxiety-disorder-the-basics
UpToDate. (n.d.). Patient education: High blood pressure emergencies (The Basics). Version 13.0. Retrieved on December 11, 2024, from https://www.uptodate.com/contents/high-blood-pressure-emergencies-the-basics
UpToDate. (n.d.). Patient education: High blood pressure in adults (The Basics). Version 24.0. Retrieved on December 11, 2024, from https://www.uptodate.com/contents/high-blood-pressure-in-adults-the-basics
UpToDate. (n.d.). Patient education: Medicines for high blood pressure (The Basics). Version 18.0. Retrieved on December 11, 2024, from https://www.uptodate.com/contents/medicines-for-high-blood-pressure-the-basics
Van Ameringen, M. (2024, October 1). Comorbid anxiety and depression in adults: Epidemiology, clinical manifestations, and diagnosis. In: M. B. Stein (Ed.). UpToDate. Retrieved on December 11, 2024, from https://www.uptodate.com/contents/comorbid-anxiety-and-depression-in-adults-epidemiology-clinical-manifestations-and-diagnosis